
We have all experienced days where our anxiety or low mood take over and life becomes heavier than usual. Additionally, most of us have jokingly (or not) used the phrase ‘I am so addicted to …’ at least once. Yet, none of this necessarily means we have reached pathological levels of dysfunction. One of the biggest questions within psychology that arises again and again is: where do we draw the line between normal human suffering and a clinical disorder? Automatically this leads to the question, why do we even need to make this distinction and what consequences does this have? If a human is suffering, does this not warrant attention, regardless of how severe the presenting symptomatology is?
We have all experienced days where our anxiety or low mood take over and life becomes heavier than usual. Additionally, most of us have jokingly (or not) used the phrase ‘I am so addicted to …’ at least once. Yet, none of this necessarily means we have reached pathological levels of dysfunction. One of the biggest questions within psychology that arises again and again is: where do we draw the line between normal human suffering and a clinical disorder? Automatically this leads to the question, why do we even need to make this distinction and what consequences does this have? If a human is suffering, does this not warrant attention, regardless of how severe the presenting symptomatology is?
Photo by Sean Benesh on Unsplash
Photo by Sean Benesh on Unsplash
A common debate in psychology today is differentiating between abnormal and normal behaviors, especially in children, who are still undergoing development. There are incredibly wide ranges of differences in development trajectories, as well as cultural, societal and contextual factors defining what ‘normal’ is (Tandon et al., 2009). This makes it extremely difficult to establish a universal standard of diagnosis, assessment and treatment. There have been many attempts made in the past to classify the distinction of what a disorder/ syndrome is. Today, one of the most commonly used systems worldwide is the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5-TR, retrieved 2023). The development of new versions of the DSM includes more than 200 researchers and clinicians, who come together to form review groups (American Psychiatric Association, retrieved 2023). The DSM-5 itself has around 300 syndromes specified with their specific symptomatology and the criteria that need to be met in order for a diagnosis to be applied (DSM-5-TR, retrieved 2023). This creates the opportunity for people to receive concrete diagnoses and have a better understanding of what is going on with them. Furthermore, it justifies using therapy in certain manners in order to treat syndromes and allows us to expand our knowledge through concrete research (APA, retrieved 2023). Yet, it does not account for the wide heterogeneity of problems people may be experiencing. If someone does not meet all the requirements for a diagnosis, they may be denied insurance coverage for treatment, even though they may still benefit from it.
Despite its usefulness, there has been criticism that the most previous review of the DSM to its latest 5th edition has resulted in a fundamental issue of validity, creating more false positives than before (Wakefield, 2016). The concern here is that ‘many millions of people with normal grief, gluttony, distractibility, worries […] will soon be mislabeled as psychiatrically sick’ (Frances, 2012, as cited by Wakefield, 2016). One point that emphasizes how large of an impact our classification system can have on society is that disorders that may not currently “exist” could become part of the next edition of the DSM. An example is that of behavioral addictions, where there is still debate about whether or not they can be added as syndromes to our diagnostic system (Petry et al., 2018). If they do become added, the question arises as to whether virtually any behavior can lead to pathological addiction? Petry et al. state regarding the possibility of an internet gaming disorder (IGD), that “as society evolves, the expression of mental disorders changes. Is technology creating new disorders or addictions?”. This begs the question: where do we draw the line at what is a disorder and what is not? If behavioral addictions such as IGD are added to the DSM, this opens the door to an overwhelming amount of other potential ‘addictions’, such as food, exercise etc.
An interesting phenomenon is the looping effect (Hacking, 2006), which describes the process through which our scientific investigation, specifically of psychological pathology, interacts with the people we are studying. By classifying individuals, we “create” certain ‘types’ of people that did not exist in the same way before. An example of this was when the first diagnosis for “Multiple Personality Disorder” (now: dissociative identity disorder) was made in 1970. Following this, more and more people began to manifest those symptoms and claimed to have up to 17 different personalities, which in turn again changed the system. The point is that just the process of classifying/ labelling people changes and affects them.
“By focusing on symptoms, rather than distinct disorders, the arbitrary line between disordered and “normal” human suffering loses its importance.”
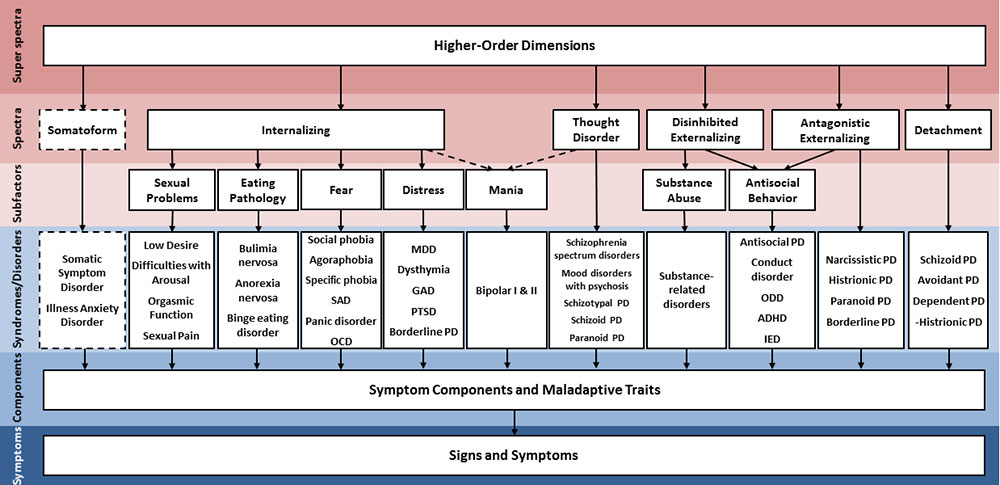
I believe a big emphasis in the future of clinical psychology diagnostics is going to be looking at clusters of symptoms and their severity, rather than specific diagnoses. An example where this is being implemented is the HiTOP model (Ruggero et al., 2019). It is a dimensional approach (ranges of symptoms with overarching concepts connecting syndromes) of classifying psychopathology rather than a categorical one as seen as the DSM-5 (clear criteria for a disorder). The image of the model shows that the dimensions are organised in a hierarchical fashion. This allows for a better picture of the complexity of syndromes and how they are related to each other. The model also integrates biological, social and psychological factors, creating a nuanced framework for treatment and research.
Although not ideal yet, it has many benefits over the DSM-5. One is being able to tackle a dimension of symptoms without labelling the individuals, allowing for more flexible treatment. Most importantly though, by focusing on symptoms, rather than distinct disorders, the arbitrary line between disordered and “normal” human suffering loses its importance. It is noteworthy to mention that there are reasons why a shift to a dimensional approach would not be easy. One of them is that labels and diagnosis are often used for insurance purposes. They help determine eligibility for reimbursement for treatment. The categories of the DSM provide a standardized language between clinical practice and insurance companies (American Psychological Association, retrieved 2023). A switch to a new system would lead to complications in coding and billing, and may call for large adaptations in insurance policies and procedures (Kilbourne et al., 2012). Here the question remains again, where, how and do we even draw the line between who receives reimbursement for treatment on the basis of being ‘abnormal enough’ and who does not?
Overall, a balance must be achieved between an overly restrictive and a too open system. On the one hand, it cannot be overly restrictive, since this makes it difficult for individuals to identify themselves with a category of pathology when they are experiencing marked distress. On the other hand, it should not be too open so that every form of human suffering is over-medicalized and heterogeneity becomes the norm within disorders. Over-medicalization refers to pathologizing normal human experiences, resulting in excessive diagnosis/interventions that may not be beneficial (Moynihan & Cassels, 2005). Heterogeneity here refers to the diversity and variation in symptoms within a disorder across individuals (Cuthbert et al., 2013). Striking a balance is an enormous challenge, especially considering the incredibly unique personality, environment, and (neuro)biology of every human being. While over-medicalizing human suffering is definitely not a far-fetched concern, in my opinion, false positives might be a small price to pay if it means avoiding false negatives. I do however also see a danger in creating new categories of disorders, as well as handing out unwarranted diagnoses. This may lead to individuals exaggerating and internalizing problems they feel they might have. The classification systems we have, have given us a lot of new research and knowledge. Perhaps it would not hurt though to take a step back from them when it comes to clinical treatment itself and invite room for alternative approaches.
Thus to conclude, the question of what is normal or abnormal is one that I do not think can be answered in general, nor do I think the answer itself should matter as much as it currently does, at least in a clinical treatment context. After all, it is rare to come across someone who has never experienced pain or distress in their lifetime. Whether or not it has come to a point of being too much to handle is something maybe everyone can only answer for themselves. <<
References
-
Association, N. B. M. (2022b). Diagnostic and Statistical Manual of Mental Disorders. Psychiatry Online. https://doi.org/10.1176/appi.books.9780890425787
-
American Psychological Association (n.d.). How is Mental Illness Diagnosed? Retrieved from https://www.apa.org/topic/mental-illness/diagnosis.
-
American Psychiatric Association. DSM. https://www.psychiatry.org/psychiatrists/practice/dsm
-
Cuthbert, B. N., & Insel, T. R. (2013). Toward the future of psychiatric diagnosis: The seven pillars of RDoC. BMC medicine, 11(1), 126. PMCID: PMC1226266. DOI: 10.1186/1741-7015-11-126.
-
Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th edition). (2014). Reference Reviews, 28(3), 36–37. https://doi.org/10.1108/rr-10-2013-0256
-
Hacking, I. (2019). Ian Hacking · Making Up People: clinical classifications · LRB 17 August 2006. London Review of Books. https://www.lrb.co.uk/the-paper/v28/n16/ian-hacking/making-up-people
-
Kilbourne, A. M., Greenwald, D. E., Bauer, M. S., Charns, M. P., & Yano, E. M. (2012). Mental health provider perspectives regarding integrated medical care for patients with serious mental illness. Administration and Policy in Mental Health and Mental Health Services Research, 39(6), 448-457. https://doi.org/10.1007/s10488-011-0365-9.
-
Moynihan, R., & Cassels, A. (2005). Selling sickness: How the world’s biggest pharmaceutical companies are turning us all into patients. Greystone Books.
-
Petry, N. M., Zajac, K., & Ginley, M. K. (2018). Behavioral Addictions as Mental Disorders: To Be or Not To Be? Annual Review of Clinical Psychology, 14(1), 399–423. https://doi.org/10.1146/annurev-clinpsy-032816-045120
-
Ruggero, C. J., Kotov, R., Hopwood, C. J., First, M. B., Clark, L. A., Skodol, A. E., Mullins-Sweatt, S. N., Patrick, C. J., Bach, B., Cicero, D. C., Docherty, A. R., Simms, L. J., Bagby, R. M., Krueger, R. F., Callahan, J. L., Chmielewski, M., Conway, C. M., De Clercq, B., Dornbach-Bender, A., . . . Zimmermann, J. (2019). Integrating the Hierarchical Taxonomy of Psychopathology (HiTOP) into clinical practice. Journal of Consulting and Clinical Psychology, 87(12), 1069–1084. https://doi.org/10.1037/ccp0000452
-
Tandon, M., Cardeli, E., & Luby, J. (2009). Internalizing Disorders in Early Childhood: A Review of Depressive and Anxiety Disorders. Child and Adolescent Psychiatric Clinics, 18(3), 593-610. doi: 10.1016/j.chc.2009.03.004
-
Wakefield, J. C. (2016). Diagnostic Issues and Controversies in DSM-5: Return of the False Positives Problem. Annual Review of Clinical Psychology, 12(1), 105–132. https://doi.org/10.1146/annurev-clinpsy-032814-112800
A common debate in psychology today is differentiating between abnormal and normal behaviors, especially in children, who are still undergoing development. There are incredibly wide ranges of differences in development trajectories, as well as cultural, societal and contextual factors defining what ‘normal’ is (Tandon et al., 2009). This makes it extremely difficult to establish a universal standard of diagnosis, assessment and treatment. There have been many attempts made in the past to classify the distinction of what a disorder/ syndrome is. Today, one of the most commonly used systems worldwide is the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5-TR, retrieved 2023). The development of new versions of the DSM includes more than 200 researchers and clinicians, who come together to form review groups (American Psychiatric Association, retrieved 2023). The DSM-5 itself has around 300 syndromes specified with their specific symptomatology and the criteria that need to be met in order for a diagnosis to be applied (DSM-5-TR, retrieved 2023). This creates the opportunity for people to receive concrete diagnoses and have a better understanding of what is going on with them. Furthermore, it justifies using therapy in certain manners in order to treat syndromes and allows us to expand our knowledge through concrete research (APA, retrieved 2023). Yet, it does not account for the wide heterogeneity of problems people may be experiencing. If someone does not meet all the requirements for a diagnosis, they may be denied insurance coverage for treatment, even though they may still benefit from it.
Despite its usefulness, there has been criticism that the most previous review of the DSM to its latest 5th edition has resulted in a fundamental issue of validity, creating more false positives than before (Wakefield, 2016). The concern here is that ‘many millions of people with normal grief, gluttony, distractibility, worries […] will soon be mislabeled as psychiatrically sick’ (Frances, 2012, as cited by Wakefield, 2016). One point that emphasizes how large of an impact our classification system can have on society is that disorders that may not currently “exist” could become part of the next edition of the DSM. An example is that of behavioral addictions, where there is still debate about whether or not they can be added as syndromes to our diagnostic system (Petry et al., 2018). If they do become added, the question arises as to whether virtually any behavior can lead to pathological addiction? Petry et al. state regarding the possibility of an internet gaming disorder (IGD), that “as society evolves, the expression of mental disorders changes. Is technology creating new disorders or addictions?”. This begs the question: where do we draw the line at what is a disorder and what is not? If behavioral addictions such as IGD are added to the DSM, this opens the door to an overwhelming amount of other potential ‘addictions’, such as food, exercise etc.
An interesting phenomenon is the looping effect (Hacking, 2006), which describes the process through which our scientific investigation, specifically of psychological pathology, interacts with the people we are studying. By classifying individuals, we “create” certain ‘types’ of people that did not exist in the same way before. An example of this was when the first diagnosis for “Multiple Personality Disorder” (now: dissociative identity disorder) was made in 1970. Following this, more and more people began to manifest those symptoms and claimed to have up to 17 different personalities, which in turn again changed the system. The point is that just the process of classifying/ labelling people changes and affects them.
“By focusing on symptoms, rather than distinct disorders, the arbitrary line between disordered and “normal” human suffering loses its importance.”
I believe a big emphasis in the future of clinical psychology diagnostics is going to be looking at clusters of symptoms and their severity, rather than specific diagnoses. An example where this is being implemented is the HiTOP model (Ruggero et al., 2019). It is a dimensional approach (ranges of symptoms with overarching concepts connecting syndromes) of classifying psychopathology rather than a categorical one as seen as the DSM-5 (clear criteria for a disorder). The image of the model shows that the dimensions are organised in a hierarchical fashion. This allows for a better picture of the complexity of syndromes and how they are related to each other. The model also integrates biological, social and psychological factors, creating a nuanced framework for treatment and research.
Although not ideal yet, it has many benefits over the DSM-5. One is being able to tackle a dimension of symptoms without labelling the individuals, allowing for more flexible treatment. Most importantly though, by focusing on symptoms, rather than distinct disorders, the arbitrary line between disordered and “normal” human suffering loses its importance. It is noteworthy to mention that there are reasons why a shift to a dimensional approach would not be easy. One of them is that labels and diagnosis are often used for insurance purposes. They help determine eligibility for reimbursement for treatment. The categories of the DSM provide a standardized language between clinical practice and insurance companies (American Psychological Association, retrieved 2023). A switch to a new system would lead to complications in coding and billing, and may call for large adaptations in insurance policies and procedures (Kilbourne et al., 2012). Here the question remains again, where, how and do we even draw the line between who receives reimbursement for treatment on the basis of being ‘abnormal enough’ and who does not?
Overall, a balance must be achieved between an overly restrictive and a too open system. On the one hand, it cannot be overly restrictive, since this makes it difficult for individuals to identify themselves with a category of pathology when they are experiencing marked distress. On the other hand, it should not be too open so that every form of human suffering is over-medicalized and heterogeneity becomes the norm within disorders. Over-medicalization refers to pathologizing normal human experiences, resulting in excessive diagnosis/interventions that may not be beneficial (Moynihan & Cassels, 2005). Heterogeneity here refers to the diversity and variation in symptoms within a disorder across individuals (Cuthbert et al., 2013). Striking a balance is an enormous challenge, especially considering the incredibly unique personality, environment, and (neuro)biology of every human being. While over-medicalizing human suffering is definitely not a far-fetched concern, in my opinion, false positives might be a small price to pay if it means avoiding false negatives. I do however also see a danger in creating new categories of disorders, as well as handing out unwarranted diagnoses. This may lead to individuals exaggerating and internalizing problems they feel they might have. The classification systems we have, have given us a lot of new research and knowledge. Perhaps it would not hurt though to take a step back from them when it comes to clinical treatment itself and invite room for alternative approaches.
Thus to conclude, the question of what is normal or abnormal is one that I do not think can be answered in general, nor do I think the answer itself should matter as much as it currently does, at least in a clinical treatment context. After all, it is rare to come across someone who has never experienced pain or distress in their lifetime. Whether or not it has come to a point of being too much to handle is something maybe everyone can only answer for themselves. <<
References
-
Association, N. B. M. (2022b). Diagnostic and Statistical Manual of Mental Disorders. Psychiatry Online. https://doi.org/10.1176/appi.books.9780890425787
-
American Psychological Association (n.d.). How is Mental Illness Diagnosed? Retrieved from https://www.apa.org/topic/mental-illness/diagnosis.
-
American Psychiatric Association. DSM. https://www.psychiatry.org/psychiatrists/practice/dsm
-
Cuthbert, B. N., & Insel, T. R. (2013). Toward the future of psychiatric diagnosis: The seven pillars of RDoC. BMC medicine, 11(1), 126. PMCID: PMC1226266. DOI: 10.1186/1741-7015-11-126.
-
Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th edition). (2014). Reference Reviews, 28(3), 36–37. https://doi.org/10.1108/rr-10-2013-0256
-
Hacking, I. (2019). Ian Hacking · Making Up People: clinical classifications · LRB 17 August 2006. London Review of Books. https://www.lrb.co.uk/the-paper/v28/n16/ian-hacking/making-up-people
-
Kilbourne, A. M., Greenwald, D. E., Bauer, M. S., Charns, M. P., & Yano, E. M. (2012). Mental health provider perspectives regarding integrated medical care for patients with serious mental illness. Administration and Policy in Mental Health and Mental Health Services Research, 39(6), 448-457. https://doi.org/10.1007/s10488-011-0365-9.
-
Moynihan, R., & Cassels, A. (2005). Selling sickness: How the world’s biggest pharmaceutical companies are turning us all into patients. Greystone Books.
-
Petry, N. M., Zajac, K., & Ginley, M. K. (2018). Behavioral Addictions as Mental Disorders: To Be or Not To Be? Annual Review of Clinical Psychology, 14(1), 399–423. https://doi.org/10.1146/annurev-clinpsy-032816-045120
-
Ruggero, C. J., Kotov, R., Hopwood, C. J., First, M. B., Clark, L. A., Skodol, A. E., Mullins-Sweatt, S. N., Patrick, C. J., Bach, B., Cicero, D. C., Docherty, A. R., Simms, L. J., Bagby, R. M., Krueger, R. F., Callahan, J. L., Chmielewski, M., Conway, C. M., De Clercq, B., Dornbach-Bender, A., . . . Zimmermann, J. (2019). Integrating the Hierarchical Taxonomy of Psychopathology (HiTOP) into clinical practice. Journal of Consulting and Clinical Psychology, 87(12), 1069–1084. https://doi.org/10.1037/ccp0000452
-
Tandon, M., Cardeli, E., & Luby, J. (2009). Internalizing Disorders in Early Childhood: A Review of Depressive and Anxiety Disorders. Child and Adolescent Psychiatric Clinics, 18(3), 593-610. doi: 10.1016/j.chc.2009.03.004
-
Wakefield, J. C. (2016). Diagnostic Issues and Controversies in DSM-5: Return of the False Positives Problem. Annual Review of Clinical Psychology, 12(1), 105–132. https://doi.org/10.1146/annurev-clinpsy-032814-112800

{kind=link}